Does Severs Disease Always Have To Have Surgical Procedures?
Overview
Sever's disease or Calcaneal apophysitis is a condition that affects children between the ages of 10 and 13 years. It is characterized by pain in one or both heels with walking. During this phase of life, growth of the bone is taking place at a faster rate than the tendons. Hence there is a relative shortening of the heel-cord compared to the leg bones. As a result, the tension the heel-cord applies to the heel bone at its insertion is very great. Moreover, the heel cord is attached to a portion of the calcaneus (heel bone) that is still immature, consisting of a mixture of bone and growing cartilage, called the calcaneal apophysis, which is prone to injury. Compounding to this is the fact that all these changes are happening in a very active child, prone to overuse. The end result is therefore an overuse syndrome of injury and inflammation at the heel where the heel cord (Achilles Tendonitis) inserts into the heel bone (Calcaneal apophysitis).
Causes
Overuse and stress on the heel bone through participation in sports is a major cause of calcaneal apophysitis. The heel?s growth plate is sensitive to repeated running and pounding on hard surfaces, resulting in muscle strain and inflamed tissue. For this reason, children and adolescents involved in soccer, track, or basketball are especially vulnerable. Other potential causes of calcaneal apophysitis include obesity, a tight Achilles tendon, and biomechanical problems such as flatfoot or a high-arched foot.
Symptoms
Sever condition causes pain at the back of the heel. The pain is increased with plantar flexion of the ankle (pushing down with the foot as if stepping on the gas), particularly against resistance. Sever condition also causes tenderness and swelling in the area of the pain.
Diagnosis
It is not difficult for a doctor to diagnose Sever's disease in a youngster or teenager. A personal history and a physical examination are usually all it takes to determine the cause of heel pain.
Non Surgical Treatment
Treatment is primarily supportive, with rest, pain management, and activity modification. Activity modifications include the addition of low-impact activities. Gel heel cups are sold over the counter and can be used intermittently to help reduce shock in the heel, as well as take tension off of the tight Achilles?s tendon complex. Proper stretching and strengthening activities should be preformed routinely even during periods of no pain. A large study showed that approximately 85% of children affected by Sever?s disease return to full activity within a two-month time period after starting treatment.
Prevention
The best way to prevent Sever's disease is to make sure that your child wears shoes that fit properly. The heel portion of the shoe should not be too tight, and there should be good padding in the heel. It may help to put extra heel pads in your child's shoes. Some children simply get too much physical activity. For example, they may play on too many teams or practice for too long. Their heel pain is a message to slow down.
Sever's disease or Calcaneal apophysitis is a condition that affects children between the ages of 10 and 13 years. It is characterized by pain in one or both heels with walking. During this phase of life, growth of the bone is taking place at a faster rate than the tendons. Hence there is a relative shortening of the heel-cord compared to the leg bones. As a result, the tension the heel-cord applies to the heel bone at its insertion is very great. Moreover, the heel cord is attached to a portion of the calcaneus (heel bone) that is still immature, consisting of a mixture of bone and growing cartilage, called the calcaneal apophysis, which is prone to injury. Compounding to this is the fact that all these changes are happening in a very active child, prone to overuse. The end result is therefore an overuse syndrome of injury and inflammation at the heel where the heel cord (Achilles Tendonitis) inserts into the heel bone (Calcaneal apophysitis).
Causes
Overuse and stress on the heel bone through participation in sports is a major cause of calcaneal apophysitis. The heel?s growth plate is sensitive to repeated running and pounding on hard surfaces, resulting in muscle strain and inflamed tissue. For this reason, children and adolescents involved in soccer, track, or basketball are especially vulnerable. Other potential causes of calcaneal apophysitis include obesity, a tight Achilles tendon, and biomechanical problems such as flatfoot or a high-arched foot.
Symptoms
Sever condition causes pain at the back of the heel. The pain is increased with plantar flexion of the ankle (pushing down with the foot as if stepping on the gas), particularly against resistance. Sever condition also causes tenderness and swelling in the area of the pain.
Diagnosis
It is not difficult for a doctor to diagnose Sever's disease in a youngster or teenager. A personal history and a physical examination are usually all it takes to determine the cause of heel pain.
Non Surgical Treatment
Treatment is primarily supportive, with rest, pain management, and activity modification. Activity modifications include the addition of low-impact activities. Gel heel cups are sold over the counter and can be used intermittently to help reduce shock in the heel, as well as take tension off of the tight Achilles?s tendon complex. Proper stretching and strengthening activities should be preformed routinely even during periods of no pain. A large study showed that approximately 85% of children affected by Sever?s disease return to full activity within a two-month time period after starting treatment.
Prevention
The best way to prevent Sever's disease is to make sure that your child wears shoes that fit properly. The heel portion of the shoe should not be too tight, and there should be good padding in the heel. It may help to put extra heel pads in your child's shoes. Some children simply get too much physical activity. For example, they may play on too many teams or practice for too long. Their heel pain is a message to slow down.
Partial Achilles Tendon Rupture Rehabilitation
Overview
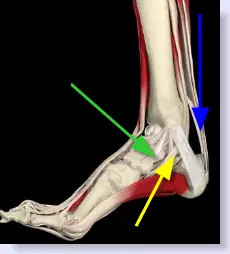 An Achilles tendon rupture is a tear in the strong fibrous cord that connects the muscles in the back of your calf to your heel bone. The tendon can rupture partially or completely. Your Achilles tendon is the largest tendon in the body and plays a critical role. In fact, you rely on it every time you move your foot. The tendon helps you point your foot down, rise on your toes and push off as you walk. An Achilles tendon rupture is a serious injury. If you suspect you have torn your Achilles - especially if you hear a pop or snap in your heel and cannot walk properly - seek medical attention immediately.
An Achilles tendon rupture is a tear in the strong fibrous cord that connects the muscles in the back of your calf to your heel bone. The tendon can rupture partially or completely. Your Achilles tendon is the largest tendon in the body and plays a critical role. In fact, you rely on it every time you move your foot. The tendon helps you point your foot down, rise on your toes and push off as you walk. An Achilles tendon rupture is a serious injury. If you suspect you have torn your Achilles - especially if you hear a pop or snap in your heel and cannot walk properly - seek medical attention immediately.
Causes
The Achilles tendon can grow weak and thin with age and lack of use. Then it becomes prone to injury or rupture. Achilles tendon rupture is more common in those with preexisting tendinitis of the Achilles tendon. Certain illnesses (such as arthritis and diabetes) and medications (such as corticosteroids and some antibiotics, including quinolones such as levofloxacin [Levaquin] and ciprofloxacin [Cipro]) can also increase the risk of rupture. Rupture most commonly occurs in the middle-aged male athlete (the weekend warrior who is engaging in a pickup game of basketball, for example). Injury often occurs during recreational sports that require bursts of jumping, pivoting, and running. Most often these are tennis, racquetball, basketball, and badminton. The injury can happen in the following situations. You make a forceful push-off with your foot while your knee is straightened by the powerful thigh muscles. One example might be starting a foot race or jumping. You suddenly trip or stumble, and your foot is thrust in front to break a fall, forcefully overstretching the tendon. You fall from a significant height or abruptly step into a hole or off of a curb.
Symptoms
If the Achilles tendon is ruptured you may experience a sudden pain in the back of your leg, as if someone had kicked you, followed by, swelling, stiffness, and difficulty to stand on tiptoe and push the leg when walking. A popping or snapping sound may be heard when the injury occurs. You may also feel a gap or depression in the tendon, just above heel bone. Ruptures usually occurs in those aged 30 - 70 years, during a sudden forceful push off from the foot. Without proper healing of the tendon, you will have a permanent limp and weakness when using the leg.
Diagnosis
Your doctor will ask you about your symptoms and examine you. He or she may also ask you about your medical history. Your doctor may ask you to do a series of movements or exercises to see how well you can move your lower leg. He or she may also examine your leg, heel and ankle and may squeeze your calf muscle to check the movement of your foot. You may need to have further tests to confirm if your tendon is torn, which may include the following. An ultrasound scan. This uses sound waves to produce an image of the inside of your leg. An MRI scan. This uses magnets and radio waves to produce images of the inside of your leg.
Non Surgical Treatment
Initial treatment for sprains and strains should occur as soon as possible. Remember RICE! Rest the injured part. Pain is the body's signal to not move an injury. Ice the injury. This will limit the swelling and help with the spasm. Compress the injured area. This again, limits the swelling. Be careful not to apply a wrap so tightly that it might act as a tourniquet and cut off the blood supply. Elevate the injured part. This lets gravity help reduce the swelling by allowing fluid and blood to drain downhill to the heart. Over-the-counter pain medication is an option. Acetaminophen (Tylenol) is helpful for pain, but ibuprofen (Motrin, Advil, Nuprin) might be better, because these medications relieve both pain and inflammation. Remember to follow the guidelines on the bottle for appropriate amounts of medicine, especially for children and teens. 
Surgical Treatment
While it is possible to treat an Achilles tendon rupture without surgery, this is not ideal since the maximum strength of the muscle and tendon rarely returns. The reason is the ends of the tendon are ruptured in a very irregular manner, almost like the ends of a paint brush. As soon as the tendon ruptures, the calf muscle (gastrocnemius muscle) continues to pull on the tendon and the end of the ruptured tendon pulls back into the leg, which is called retraction. Once the tendon retracts, it is never possible to get sufficient strength back without surgery, because the muscle no longer functions at the correct biomechanical length and is now stretched out. There are patients for whom surgery cannot be performed, in particular, due to existing medical conditions that may add to potential for complications following surgery. For these patients, a specially designed boot that positions the foot correctly and takes the pressure and tension off the muscle and tendon is used. Most importantly, a cast is never used because it causes permanent shrinkage (atrophy) of the calf muscle. The special boot permits pressure on the foot with walking. The boot also has a hinge to permit movement of the ankle. Many studies of Achilles tendon ruptures have shown that this movement of the foot in the boot while walking is ideal for tendon healing. If surgery is not recommended, it is essential to obtain special tests to check that the ends of the tendon are lying next to each other so that healing can occur. The best test to do this is an ultrasound and not an MRI.
Prevention
To help reduce your chance of getting Achilles tendon rupture, take the following steps. Do warm-up exercises before an activity and cool down exercises after an activity. Wear proper footwear. Maintain a healthy weight. Rest if you feel pain during an activity. Change your routine. Switch between high-impact activities and low-impact activities. Strengthen your calf muscle with exercises.
Leg Length Discrepancy And Running Performance
Overview
The majority of people in the world actually have some degree of leg length discrepancy, up to 2cm. One study found that only around 1/4 of people have legs of equal lengths. LLD of greater than 2cm is relatively rare, however, and the greater the discrepancy, the greater the chances of having a clinical problem down the road. A limp generally begins when LLD exceeds 2cm and becomes extremely noticeable above 3cm. When patients with LLD develop an abnormal gait, one of the debilitating clinical features can be fatigue because of the relatively high amount of energy needed to walk in the new, inefficient way. Poliomyelitis, or polio, as it is more commonly known, used to account for around 1/3 of all cases of LLD, but due to the effectiveness of polio vaccines, it now represents a negligible cause of the condition. Functional LLD, described above, usually involves treatment focused on the hip, pelvis, and/or lower back, rather than the leg. If you have been diagnosed with functional LLD or pelvic obliquity, please ask your orthopaedic surgeon for more information about treatment of these conditions.
Causes
A patient?s legs may be different lengths for a number of reasons, including a broken leg bone may heal in a shorter position, particularly if the injury was severe. In children, broken bones may grow faster for a few years after they heal, resulting in one longer leg. If the break was near the growth center, slower growth may ensue. Children, especially infants, who have a bone infection during a growth spurt may have a greater discrepancy. Inflammation of joints, such as juvenile arthritis during growth, may cause unequal leg length. Compensation for spinal or pelvic scoliosis. Bone diseases such as Ollier disease, neurofibromatosis, or multiple hereditary exostoses. Congenital differences.
Symptoms
Often there are few or no symptoms prior to the age of 25-35. The most common symptom is chronic lower back pain, but also is frequently middle and upper back pain. Same-sided and repeated injury or pain to the hip, knee and/or ankle is also a hallmark of a long-standing untreated LLD. It is not uncommon to have buttock or radiating hip pain that is non-dermatomal (not from a disc) and tends to go away when lying down.
Diagnosis
Asymmetry is a clue that a LLD is present. The center of gravity will shift to the short limb side and patients will try to compensate, displaying indications such as pelvic tilt, lumbar scoliosis, knee flexion, or unilateral foot pronation. Asking simple questions such as, "Do you favor one leg over the other?" or, "Do you find it uncomfortable to stand?" may also provide some valuable information. Performing a gait analysis will yield some clues as to how the patient compensates during ambulation. Using plantar pressure plates can indicate load pressure differences between the feet. It is helpful if the gait analysis can be video-recorded and played back in slow motion to catch the subtle aspects of movement.
Non Surgical Treatment
Treatment of leg length inequality involves many different approaches, such as orthotics, epiphysiodesis, shortening, and lengthening, which can be used alone or combined in an effort to achieve equalization of leg lengths. Leg length inequality of 2 cm or less is usually not a functional problem. Often, leg length can be equalized with a shoe lift, which usually corrects about two thirds of the leg length inequality. Up to 1 cm can be inserted in the shoe. For larger leg length inequalities, the shoe must be built up. This needs to be done for every shoe worn, thus limiting the type of shoe that the patient can wear. Leg length inequalities beyond 5 cm are difficult to treat with a shoe lift. The shoe looks unsightly, and often the patient complains of instability with such a large lift. A foot-in-foot prosthesis can be used for larger leg length inequalities. This is often done as a temporizing measure for young children with significant leg length inequalities. The prosthesis is bulky, and a fixed equinus contracture may result.

Surgical Treatment
Leg shortening is employed when LLD is severe and when a patient has already reached skeletal maturity. The actual surgery is called an osteotomy , which entails the removal of a small section of bone in the tibia (shinbone) and sometimes the fibula as well, resulting in the loss of around an inch in total height. Leg lengthening is a difficult third option that has traditionally had a high complication rate. Recently, results have improved somewhat with the emergence of a technique known as callotasis , in which only the outer portion of the bone (the cortex ) is cut, (i.e. a corticotomy ). This allows the bone to be more easily lengthened by an external fixation device that is attached to either side of the cut bone with pins through the skin. The ?ex-fix,' as it is sometimes called, is gradually adjusted by an orthopaedic surgeon, and healing can occur at the same time that the leg is being distracted , or lengthened over time. Unlike epiphysiodesis, leg lengthening procedures can be performed at almost any skeletal or chronological age.
The majority of people in the world actually have some degree of leg length discrepancy, up to 2cm. One study found that only around 1/4 of people have legs of equal lengths. LLD of greater than 2cm is relatively rare, however, and the greater the discrepancy, the greater the chances of having a clinical problem down the road. A limp generally begins when LLD exceeds 2cm and becomes extremely noticeable above 3cm. When patients with LLD develop an abnormal gait, one of the debilitating clinical features can be fatigue because of the relatively high amount of energy needed to walk in the new, inefficient way. Poliomyelitis, or polio, as it is more commonly known, used to account for around 1/3 of all cases of LLD, but due to the effectiveness of polio vaccines, it now represents a negligible cause of the condition. Functional LLD, described above, usually involves treatment focused on the hip, pelvis, and/or lower back, rather than the leg. If you have been diagnosed with functional LLD or pelvic obliquity, please ask your orthopaedic surgeon for more information about treatment of these conditions.
Causes
A patient?s legs may be different lengths for a number of reasons, including a broken leg bone may heal in a shorter position, particularly if the injury was severe. In children, broken bones may grow faster for a few years after they heal, resulting in one longer leg. If the break was near the growth center, slower growth may ensue. Children, especially infants, who have a bone infection during a growth spurt may have a greater discrepancy. Inflammation of joints, such as juvenile arthritis during growth, may cause unequal leg length. Compensation for spinal or pelvic scoliosis. Bone diseases such as Ollier disease, neurofibromatosis, or multiple hereditary exostoses. Congenital differences.
Symptoms
Often there are few or no symptoms prior to the age of 25-35. The most common symptom is chronic lower back pain, but also is frequently middle and upper back pain. Same-sided and repeated injury or pain to the hip, knee and/or ankle is also a hallmark of a long-standing untreated LLD. It is not uncommon to have buttock or radiating hip pain that is non-dermatomal (not from a disc) and tends to go away when lying down.
Diagnosis
Asymmetry is a clue that a LLD is present. The center of gravity will shift to the short limb side and patients will try to compensate, displaying indications such as pelvic tilt, lumbar scoliosis, knee flexion, or unilateral foot pronation. Asking simple questions such as, "Do you favor one leg over the other?" or, "Do you find it uncomfortable to stand?" may also provide some valuable information. Performing a gait analysis will yield some clues as to how the patient compensates during ambulation. Using plantar pressure plates can indicate load pressure differences between the feet. It is helpful if the gait analysis can be video-recorded and played back in slow motion to catch the subtle aspects of movement.
Non Surgical Treatment
Treatment of leg length inequality involves many different approaches, such as orthotics, epiphysiodesis, shortening, and lengthening, which can be used alone or combined in an effort to achieve equalization of leg lengths. Leg length inequality of 2 cm or less is usually not a functional problem. Often, leg length can be equalized with a shoe lift, which usually corrects about two thirds of the leg length inequality. Up to 1 cm can be inserted in the shoe. For larger leg length inequalities, the shoe must be built up. This needs to be done for every shoe worn, thus limiting the type of shoe that the patient can wear. Leg length inequalities beyond 5 cm are difficult to treat with a shoe lift. The shoe looks unsightly, and often the patient complains of instability with such a large lift. A foot-in-foot prosthesis can be used for larger leg length inequalities. This is often done as a temporizing measure for young children with significant leg length inequalities. The prosthesis is bulky, and a fixed equinus contracture may result.
Surgical Treatment
Leg shortening is employed when LLD is severe and when a patient has already reached skeletal maturity. The actual surgery is called an osteotomy , which entails the removal of a small section of bone in the tibia (shinbone) and sometimes the fibula as well, resulting in the loss of around an inch in total height. Leg lengthening is a difficult third option that has traditionally had a high complication rate. Recently, results have improved somewhat with the emergence of a technique known as callotasis , in which only the outer portion of the bone (the cortex ) is cut, (i.e. a corticotomy ). This allows the bone to be more easily lengthened by an external fixation device that is attached to either side of the cut bone with pins through the skin. The ?ex-fix,' as it is sometimes called, is gradually adjusted by an orthopaedic surgeon, and healing can occur at the same time that the leg is being distracted , or lengthened over time. Unlike epiphysiodesis, leg lengthening procedures can be performed at almost any skeletal or chronological age.
What To Do For Flat Feet In Adults
Overview PTTD is a common condition treated by foot and ankle specialists. Although there is a role for surgical treatment of PTTD, conservative care often can prevent or delay surgical intervention. Decreasing inflammation and stabilizing the affected joints associated with the posterior tibial tendon can decrease pain and increase functional levels. With many different modalities available, aggressive nonoperative methods should be considered in the treatment of PTTD, including early immobilization, the use of long-term bracing, physical therapy, and anti-inflammatory medications. If these methods fail, proper evaluation and work-up for surgical intervention should be employed.  Causes Causes of an adult acquired flatfoot may include Neuropathic foot (Charcot foot) secondary to Diabetes mellitus, Leprosy, Profound peripheral neuritis of any cause. Degenerative changes in the ankle, talonavicular or tarsometatarsal joints, or both, secondary to Inflammatory arthropathy, Osteoarthropathy, Fractures, Acquired flatfoot resulting from loss of the supporting structures of the medial longitudinal arch. Dysfunction of the tibialis posterior tendon Tear of the spring (calcaneoanvicular) ligament (rare). Tibialis anterior rupture (rare). Painful flatfoot can have other causes, such as tarsal coalition, but as such a patient will not present with a change in the shape of the foot these are not included here. Symptoms Not everyone with adult flatfoot has problems with pain. Those who do usually experience it around the ankle or in the heel. The pain is usually worse with activity, like walking or standing for extended periods. Sometimes, if the condition develops from arthritis in the foot, bony spurs along the top and side of the foot develop and make wearing shoes more painful. Diabetic patients need to watch for swelling or large lumps in the feet, as they may not notice any pain. They are also at higher risk for developing significant deformities from their flatfoot. Diagnosis Examination by your foot and ankle specialist can confirm the diagnosis for most patients. An ultrasound exam performed in the office setting can evaluate the status of the posterior tibial tendon, the tendon which is primarily responsible for supporting the arch structure of the foot. Non surgical Treatment Orthotic or anklebrace, Over-the-counter or custom shoe inserts to position the foot and relieve pain are the most common non-surgical treatment option. Custom orthotics are often suggested if the shape change of the foot is more severe. An ankle brace (either over-the-counter or custom made) is another option that will help to ease tendon tension and pain. Boot immobilization. A walking boot supports the tendon and allows it to heal. Activity modifications. Depending on what we find, we may recommend limiting high-impact activities, such as running, jumping or court sports, or switching out high-impact activities for low-impact options for a period of time. Ice and anti-inflammatory medications. These may be given as needed to decrease your symptoms.
Causes Causes of an adult acquired flatfoot may include Neuropathic foot (Charcot foot) secondary to Diabetes mellitus, Leprosy, Profound peripheral neuritis of any cause. Degenerative changes in the ankle, talonavicular or tarsometatarsal joints, or both, secondary to Inflammatory arthropathy, Osteoarthropathy, Fractures, Acquired flatfoot resulting from loss of the supporting structures of the medial longitudinal arch. Dysfunction of the tibialis posterior tendon Tear of the spring (calcaneoanvicular) ligament (rare). Tibialis anterior rupture (rare). Painful flatfoot can have other causes, such as tarsal coalition, but as such a patient will not present with a change in the shape of the foot these are not included here. Symptoms Not everyone with adult flatfoot has problems with pain. Those who do usually experience it around the ankle or in the heel. The pain is usually worse with activity, like walking or standing for extended periods. Sometimes, if the condition develops from arthritis in the foot, bony spurs along the top and side of the foot develop and make wearing shoes more painful. Diabetic patients need to watch for swelling or large lumps in the feet, as they may not notice any pain. They are also at higher risk for developing significant deformities from their flatfoot. Diagnosis Examination by your foot and ankle specialist can confirm the diagnosis for most patients. An ultrasound exam performed in the office setting can evaluate the status of the posterior tibial tendon, the tendon which is primarily responsible for supporting the arch structure of the foot. Non surgical Treatment Orthotic or anklebrace, Over-the-counter or custom shoe inserts to position the foot and relieve pain are the most common non-surgical treatment option. Custom orthotics are often suggested if the shape change of the foot is more severe. An ankle brace (either over-the-counter or custom made) is another option that will help to ease tendon tension and pain. Boot immobilization. A walking boot supports the tendon and allows it to heal. Activity modifications. Depending on what we find, we may recommend limiting high-impact activities, such as running, jumping or court sports, or switching out high-impact activities for low-impact options for a period of time. Ice and anti-inflammatory medications. These may be given as needed to decrease your symptoms.  Surgical Treatment Surgical intervention for adult acquired flatfoot is appropriate when there is pain and swelling, and the patient notices that one foot looks different than the other because the arch is collapsing. As many as three in four adults with flat feet eventually need surgery, and it?s better to have the joint preservation procedure done before your arch totally collapses. In most cases, early and appropriate surgical treatment is successful in stabilizing the condition.
Surgical Treatment Surgical intervention for adult acquired flatfoot is appropriate when there is pain and swelling, and the patient notices that one foot looks different than the other because the arch is collapsing. As many as three in four adults with flat feet eventually need surgery, and it?s better to have the joint preservation procedure done before your arch totally collapses. In most cases, early and appropriate surgical treatment is successful in stabilizing the condition.